
She thought the hardest part was over—accepting the end of their journey to having children, armed with birth control and careful plans. But when the IUD unleashed a storm of anxiety and panic attacks she thought she’d left behind, the fragile balance of their lives shattered, forcing them both to face fears far deeper than they expected.
Now, standing at a crossroads of trust and vulnerability, they grapple with a decision that tests their bond. Her plea for his vasectomy is no longer hypothetical—it’s an urgent need for peace, yet his hesitation hangs heavy between them, a silent battle of love, sacrifice, and the uncertain path ahead.

Would you divorce your husband for not getting a vasectomy?

Dr. Lori Gottlieb, a psychotherapist specializing in relationships and self-discovery, often discusses the importance of clearly defined boundaries and navigating conflicting needs in long-term partnerships. In this situation, the conflict centers on shared responsibility versus individual autonomy, especially concerning medical decisions.
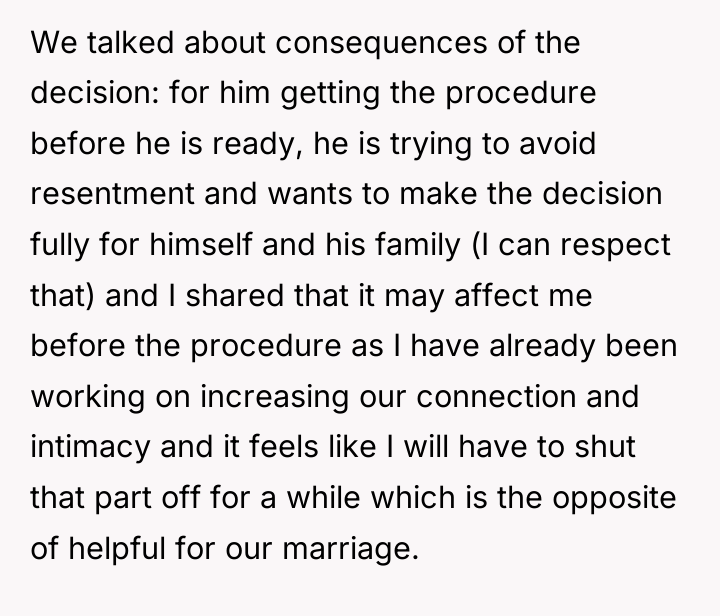
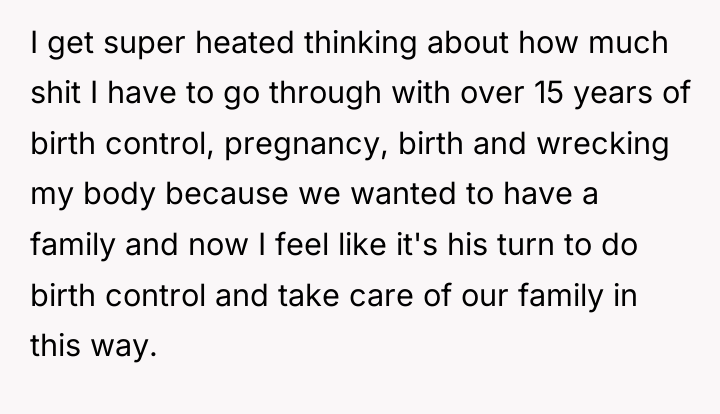
The original poster (OP) is expressing a valid feeling of ‘reproductive exhaustion’ and a strong desire for equitable emotional and physical labor distribution, which is a common theme in modern partnerships where women disproportionately manage contraception. The OP’s reaction—feeling that it is now the husband’s ‘turn’—is rooted in a desire for fairness after years of physical consequence (pregnancy, IUD side effects). However, the husband is presenting a genuine barrier: trauma linked to medical procedures. Forcing the procedure before he is ready, even with good intentions, risks creating the very resentment (as he fears) that undermines marital connection.
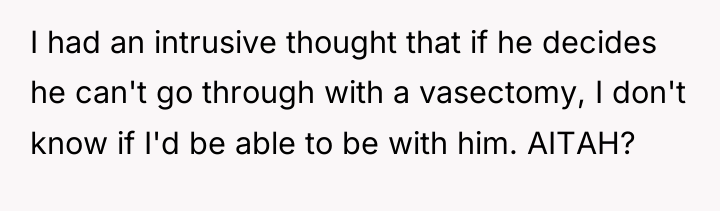
The OP’s intrusive thought that she might leave him if he does not proceed indicates that this issue has moved beyond a logistical disagreement into a fundamental alignment test regarding partnership responsibilities. The most constructive path forward involves respecting his timeline for therapy and procedural readiness while agreeing to stringent, temporary measures (like abstinence) that protect the OP from unintended pregnancy. Future planning should focus on mutual support for his trauma work, recognizing that true partnership involves supporting each other through necessary but difficult personal processes.
THE COMMENTS SECTION WENT WILD – REDDIT HAD *A LOT* TO SAY ABOUT THIS ONE.

While his fear is completely understandable, it takes two to tango and after 15 years, it’s his turn to carry the torch.

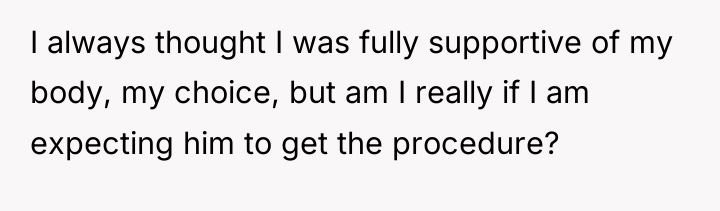
The individual is experiencing significant distress due to a perceived imbalance in reproductive responsibility, feeling they have carried the physical and emotional burden of contraception and childbearing for over a decade. Their core conflict lies between their belief in bodily autonomy and the expectation that their partner must now undergo a vasectomy to maintain equality in this shared responsibility.
Given the depth of feeling that this issue is a dealbreaker, the core question remains: When one partner has historically managed all risks associated with reproduction, is it fair to demand the other partner undergo a permanent medical procedure to balance that load, or does the partner with the medical trauma history have the primary right to dictate the timing and necessity of irreversible bodily changes?





{kind=link}