
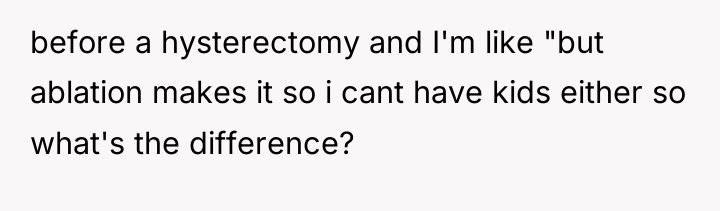
The individual was at a triage area for a scheduled hysterectomy consultation when a nurse began questioning the necessity of the procedure for managing pain and heavy bleeding. The individual explained that the pain was debilitating, significantly impacting daily life, including walking their child to school, and that the bleeding required careful scheduling of family activities.
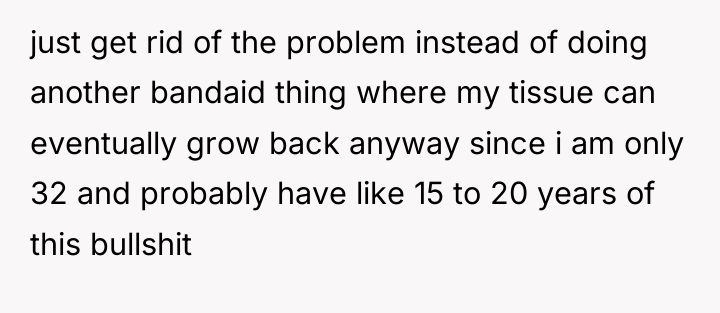
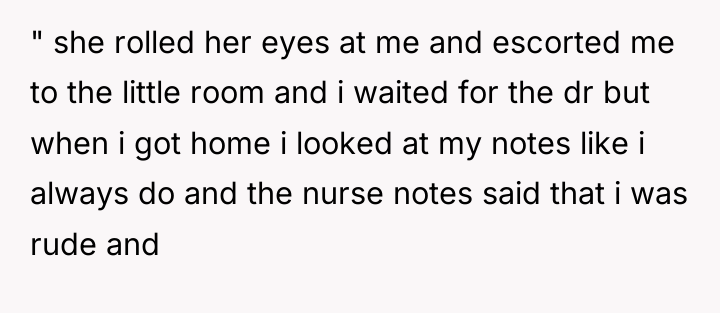
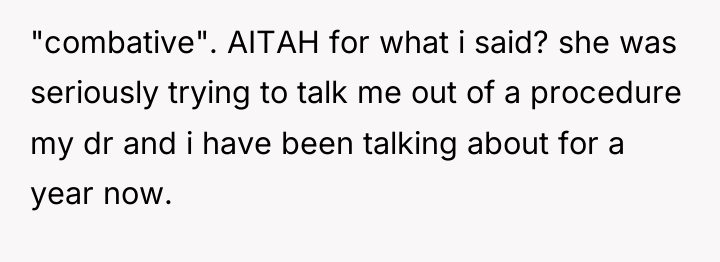
The questioning continued with hypotheticals about future relationships and childbearing desires, to which the individual gave short, definitive answers, such as suggesting their existing children could be adopted if a future partner wanted a child. When the nurse suggested less permanent solutions like birth control or endometrial ablation instead of hysterectomy, the individual argued these were only temporary fixes for a problem they wanted permanently solved. Upon returning home and checking their medical notes, the individual discovered the nurse had documented their behavior as rude and combative, leading them to question if their responses were inappropriate.
AITAH for making the nurse at my hysterectomy pre-op appointment feel stupid?

As renowned psychologist Dr. Harriet Lerner states, “When we try to make someone else responsible for our feelings, we give away our personal power.” While Lerner often speaks about interpersonal dynamics, this principle applies to the medical setting: the patient holds the power over their body and medical choices, even when facing resistance or questioning from providers.
The situation highlights a common dynamic where patients, particularly women seeking gynecological procedures, face skepticism or gatekeeping from medical professionals. The OP’s decision to pursue a hysterectomy suggests a long history of suffering that has led them to reject temporary solutions, a stance that is medically understandable when pain is truly debilitating. However, the nurse’s line of questioning, while perhaps rooted in standard risk assessment or institutional bias against permanent procedures, was perceived as confrontational and dismissive. The OP’s responses—shrugging off the hypothetical divorce scenario and directly challenging the rationale for less invasive procedures—were a natural defense mechanism against feeling invalidated.
The OP’s actions, while emotionally charged, were an attempt to firmly assert autonomy over their treatment plan after previous attempts at relief failed. In the future, the OP could manage such encounters more effectively by stating their position calmly but firmly, for example: “I understand your concerns, but my doctor and I have thoroughly reviewed all options, and this is the plan we have agreed upon for my quality of life.” This acknowledges the nurse’s role without inviting prolonged debate over settled decisions.
HERE’S HOW REDDIT BLEW UP AFTER HEARING THIS – PEOPLE COULDN’T BELIEVE IT.
The original poster (OP) is facing a dilemma stemming from a perceived conflict between advocating firmly for their necessary medical treatment and adhering to expected social politeness during a medical appointment. The OP felt the nurse was attempting to derail a medically supported plan, leading to defensive and blunt responses regarding future family scenarios and treatment alternatives.
The central question is whether the OP’s direct and frustrated communication style, in response to what felt like unwarranted probing and dismissal of their chosen treatment path, justified the nurse’s negative documentation. Readers must weigh the OP’s right to advocate for their complex health needs against the professional expectation of maintaining civil dialogue with medical staff.







{kind=link}