
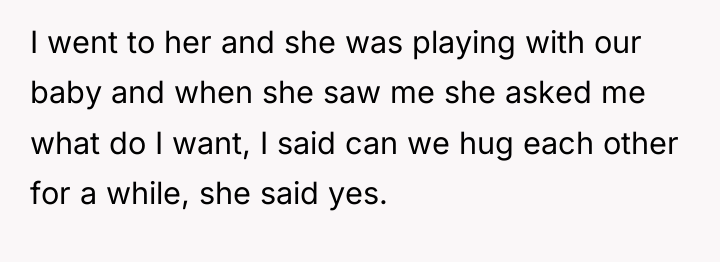
In the quiet storm of new parenthood, a husband’s heart is torn between fear and fierce love. His wife, overwhelmed by the raw and uncharted changes of childbirth, lashes out in ways he has never seen before. Despite the harsh words and the pain, he refuses to abandon the family they created, choosing instead to stand steadfastly by her side, ready to bear whatever comes for the sake of their love and their baby.
Amidst the confusion and the flood of advice, he grasps for hope and understanding, learning about the unseen battles his wife faces. Determined to help her heal, he reaches out to family, breaking his silence and inviting support. His courage to seek help marks the beginning of a fragile journey toward recovery, driven by unwavering devotion and the promise of brighter days ahead.

Update: Aita for telling my wife she’s perfect the way she is after she gave birth a month ago which resulted in her lashing onto me?

Dr. Shoshana Sznitman, a specialist in perinatal mental health, often emphasizes that acute, aggressive statements made by new mothers are frequently expressions of overwhelming emotional deregulation, fear, or physical discomfort, rather than true intent to harm. Such statements should be treated as urgent calls for support, not merely relationship insults.
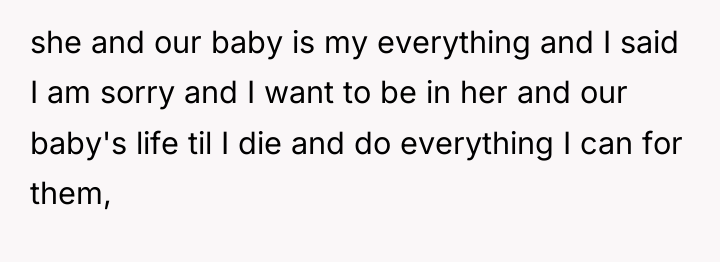
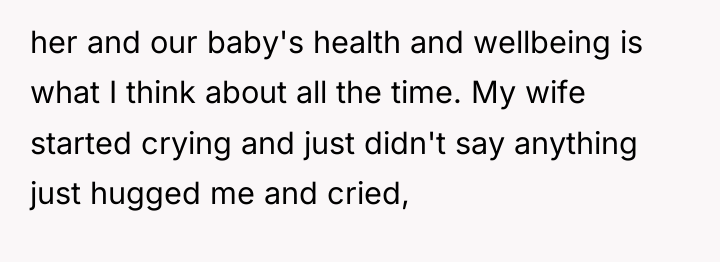
The poster demonstrated high emotional labor and commitment by immediately pivoting toward comfort and reassurance after reviewing community feedback. His prioritization of reaffirming love and commitment provided the necessary emotional anchor for his wife, leading to a release of tension evidenced by her crying and eventual sleep. However, deferring medical consultation until the mother-in-law arrives introduces a risk. Postpartum mood disorders (PPD) and postpartum psychosis (PPP) can escalate rapidly. While involving extended family for immediate logistical and emotional support is beneficial, it should not replace professional clinical assessment, especially when concerning threats or severe behavioral shifts occur.
The poster’s decision to seek education and remain vigilantly supportive is appropriate for immediate crisis de-escalation. Moving forward, the constructive recommendation is to establish a clear boundary between emotional support and clinical management. While waiting for the mother-in-law, the poster should have a low-barrier path to contacting an emergency mental health line or labor and delivery ward if his wife’s agitation returns or if she shows signs of not bonding with the baby upon waking. Sustained reassurance is vital, but clinical oversight is non-negotiable during this vulnerable period.
THIS STORY SHOOK THE INTERNET – AND REDDITORS DIDN’T HOLD BACK.
:- >
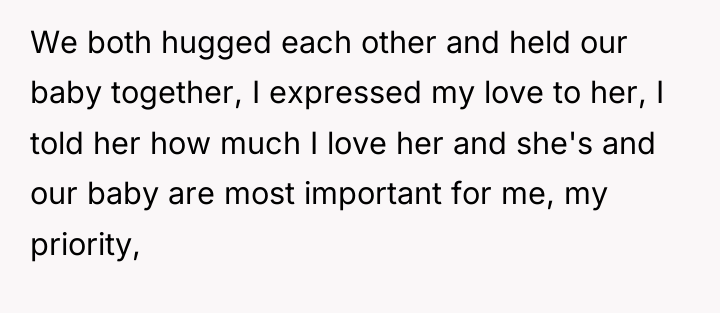
The individual demonstrated a deep commitment to his wife and newborn child, prioritizing staying with them despite the extreme stress indicated by his wife’s volatile emotional state and threat of physical action. His central conflict involved balancing the immediate need to soothe his wife against external suggestions to leave, choosing steadfast support rooted in his love and belief that her actions stemmed from suffering rather than malice.
Given the acute emotional distress and potential postpartum complications, should the focus remain solely on emotional comfort and family support, or was involving medical professionals immediately a necessary step regardless of the mother-in-law’s impending arrival?




{kind=link}