
The original poster (OP) is facing a disagreement with her husband regarding the choice of pharmacy for their medical prescriptions. The core conflict arose when the husband, who is unemployed and covered under the OP’s health insurance plan, proposed moving his prescriptions to a small, local pharmacy in their town.
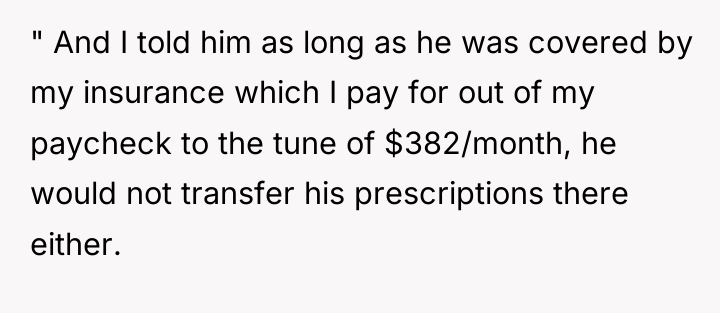
The OP immediately refused to transfer her own prescriptions to this local business, citing the pharmacy owner’s and the business’s strong pro-Trump and MAGA political leanings. When the husband insisted on transferring only his prescriptions, the OP stated he could not do so either, arguing that since she pays $382 monthly for the insurance covering him, she has the right to dictate which businesses their shared coverage supports. This left the OP wondering if her stance makes her the ‘asshole’ in the situation.

Aitah for telling my husband he can’t use a pro Trump/MAGA pharmacy?
According to Dr. Rowan Cooper, a specialist in family financial dynamics, ‘Financial contribution establishes a clear line of equity, but dictating personal consumption choices based on moral alignment often trespasses into the realm of personal autonomy, which can be highly corrosive to partnership trust.’
The OP’s argument rests on clear financial leverage: she pays for the insurance, therefore she controls its parameters. This is a strong boundary assertion regarding resource allocation. However, the husband’s motivation—moving prescriptions—is likely driven by convenience or a desire to support a local business, even if he is not ideologically extreme himself. The OP is extending her right to choose where *she* shops into a right to control where *he* seeks medical services under her plan. This distinction between controlling the insurance premium versus controlling the downstream service provider is crucial.
While setting boundaries around shared financial resources is healthy, controlling a spouse’s access to services based on moral vetting of third-party vendors can be perceived as overly controlling, particularly when the spouse is unemployed. A professional path forward might involve the OP maintaining her boundary regarding her own prescriptions while negotiating a compromise for the husband, perhaps by agreeing to cover an increased deductible or co-pay if he chooses a pharmacy outside the preferred network, thereby separating his choice from her financial support of the objectionable business.
AFTER THIS STORY DROPPED, REDDIT WENT INTO MELTDOWN MODE – CHECK OUT WHAT PEOPLE SAID.


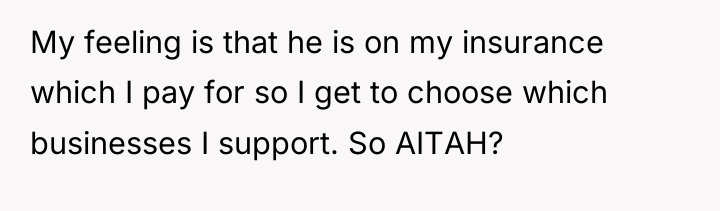
The OP is currently in a conflict where her personal political values and desire to avoid financially supporting businesses whose views she strongly opposes are directly clashing with her husband’s desire for convenience or preference in using a local service provider. Her position centers on her financial contribution to the shared healthcare plan, which she views as granting her veto power over how that coverage is utilized.
The central question is whether one partner’s financial contribution to a shared benefit, such as health insurance, grants them the unilateral authority to dictate the usage choices of the other partner, especially when those choices involve personal, non-essential business preferences. Readers must consider the balance between financial contribution and marital autonomy in shared benefits.




{kind=link}