
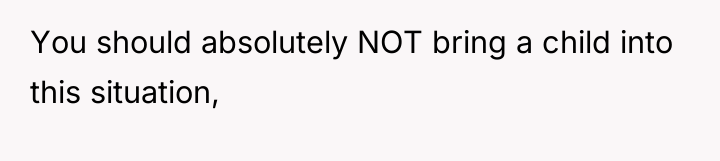
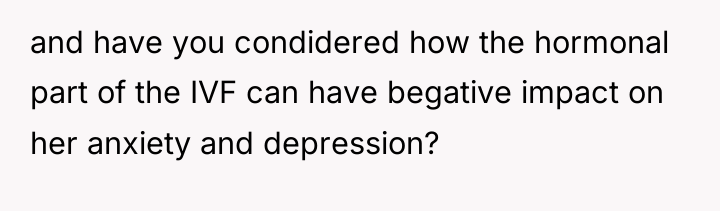
In the quiet shadows of their shared nights, a husband watches his wife battle the invisible storms of anxiety and trauma. Bound by love and respect for her painful past, he honors the unspoken lines she’s drawn, even as the relentless weight of IVF and hormone fluctuations fray the fragile threads of their intimacy.
But now, as medication ushers her into a deep, restless sleep, those boundaries blur in the darkness. Unseen desires emerge from the depths of her subconscious, igniting a silent struggle between fear, hope, and the desperate longing for connection in a world where healing feels both near and heartbreakingly out of reach.

AITAH (34M/29F) Advice need on how to handle this situation with my wife.
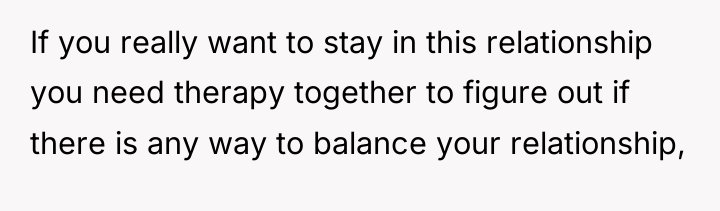
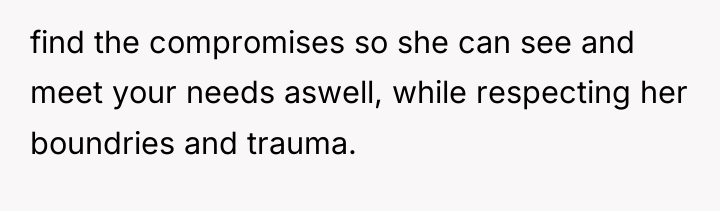
As renowned researcher Dr. Brené Brown explains, “Boundaries are the distance at which I can love you and me simultaneously.” This situation presents a complex conflict where two valid needs—the wife’s need for safety and respected boundaries regarding her trauma history, and the husband’s need for intimacy and feeling wanted—are actively colliding, making it impossible for both parties to feel fully loved and respected at the same time.
The core issue lies in the wife’s involuntary behavior triggered by new medication. While the OP correctly upholds the established boundary by stopping contact and informing her, he is experiencing a significant emotional burden, feeling repeatedly rejected. The wife’s amnesia regarding these events means she cannot offer the reciprocal validation or understanding of his hurt that he needs, leading to feelings of isolation. This dynamic creates a caretaking exhaustion for the OP where his emotional needs are consistently unmet because the only window for intimacy is one he must actively close for safety reasons.
The OP’s impulse to stop telling her or to sleep separately stems from a need to manage his own emotional pain. Sleeping separately is a temporary, healthy boundary for the OP to prevent nightly rejection. However, stopping communication about the events completely risks undermining the wife’s trust if she later learns about her sleep-sex behaviors from another source. The most constructive approach is for the OP to communicate his feelings (not the actions themselves, which she cannot process) during the day, perhaps with her therapist’s guidance, and to establish a safe physical boundary, such as sleeping in separate rooms temporarily, until the medication dosage stabilizes or a new joint agreement can be reached with professional support.
HERE’S HOW REDDIT BLEW UP AFTER HEARING THIS – PEOPLE COULDN’T BELIEVE IT.


The original poster (OP) is experiencing significant emotional distress, feeling rejected and alone because the only time his wife shows sexual interest is when she is under the influence of medication causing her to act without conscious awareness. This directly conflicts with the established boundary, rooted in her history of trauma, which prohibits sexual contact when she is asleep.
Given that the OP is being asked to repeatedly enforce a boundary against his own desire for intimacy, should he continue to wake and inform his wife of these nighttime actions despite the emotional toll it takes on him, or should he prioritize his own emotional needs by sleeping separately to avoid the repeated nightly rejection?



{kind=link}