
In the quiet routine of a physical therapy clinic, an ordinary check-in became charged with unexpected tension. A returning patient, silent and brusque, shattered the calm by tossing a bill like a weapon, their cold indifference cutting deeper than words. The front office worker, taken aback yet composed, faced this silent storm with a steady heart.
Behind the curt exchange and biting remarks lay a fragile human moment—an apology wrapped in sarcasm, a challenge met with quiet grace. This brief collision of tempers revealed the unspoken struggles beneath everyday interactions, reminding us how thin the line can be between patience and pain.

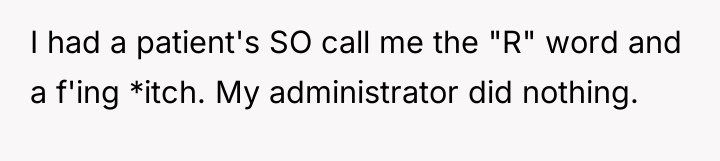
AITA for asking a patient why they threw something at me?
According to organizational psychologist Dr. Christine Porath, who has extensively researched incivility in the workplace, interactions such as these—where simple disrespect is normalized—can significantly degrade employee well-being and performance. The patient’s initial action of tossing the bill, followed by the dismissive and passive-aggressive remark about New England, clearly establishes a pattern of low-level incivility or bullying behavior directed at the front-office employee.
The office worker correctly identified and called out the initial behavior, which is an important step in boundary setting. However, the patient demonstrated an immediate resistance to accountability, attempting to deflect by minimizing the action (“If I had thrown it at you it would have hit you”). When the therapist intervened, the patient escalated the situation further, refusing to accept the premise of respectful interaction, culminating in the aggressive outburst and explicit verbal abuse toward the initial staff member. This pattern indicates a strong sense of entitlement and an inability to manage frustration within professional parameters.
The therapist’s decision to terminate services was appropriate given the patient’s explicit aggression and refusal to adhere to basic behavioral standards, especially considering the potential safety risk of dealing with an already volatile individual. For future situations, staff should be supported in enforcing a zero-tolerance policy for abusive language immediately. A constructive approach is to address only the behavior, not the person: ‘I cannot continue this conversation while you are yelling,’ rather than engaging in a debate about whose fault the interaction is.
HERE’S HOW REDDIT BLEW UP AFTER HEARING THIS – PEOPLE COULDN’T BELIEVE IT.
The person in this situation experienced a clear lack of professional respect, leading to escalating conflict when they questioned the patient’s disrespectful action. The central conflict lies between the necessity of maintaining professional boundaries and service standards versus the patient’s entitlement to care, regardless of their conduct.
Was the staff member justified in speaking up about the initial disrespectful act, thereby potentially jeopardizing the patient’s necessary physical therapy appointment, or should they have absorbed the slight to ensure continuity of care?




{kind=link}