
The anticipation of new life often brings joy and hope, but beneath that excitement lies the fragile reality of birth’s unpredictable nature. For one father, the moment his son was born was a whirlwind of fear and urgency—a race against time as his baby, struggling for breath, was rushed into emergency care. Holding his wife’s hand through the haze of anesthesia, he faced the unbearable silence of a newborn who refused to cry, each second stretching into an agonizing eternity.
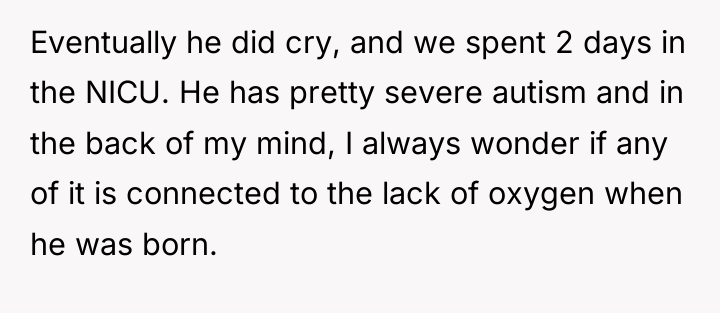
That first cry eventually came, a fragile sound that marked the beginning of a tough journey filled with uncertainty and challenges. Two days in the NICU became a small glimpse into a lifelong path marked by love, resilience, and the unspoken question that haunts every parent—could those first moments in the hospital have shaped the future in ways they cannot yet understand? Through it all, hope and strength remain, woven into the story of a family learning to navigate the unknown.

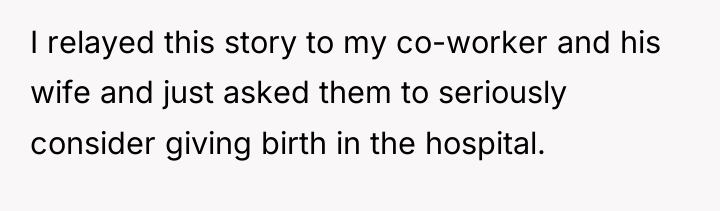
AITA for telling my co-worker and his pregnant wife the risks of having a home birth?

Dr. Brené Brown, a research professor known for her work on vulnerability and shame, often discusses how sharing difficult personal stories can be a powerful act of connection, but it must be done with careful consideration of the receiver’s capacity and context. In this situation, while the narrator’s intent is rooted in love and the avoidance of future pain (a form of protective vulnerability), the delivery is inappropriate for the timing and recipient group.
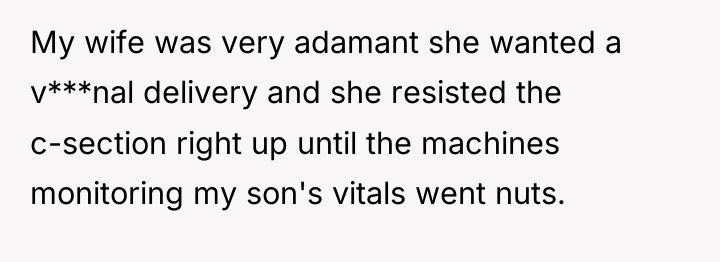
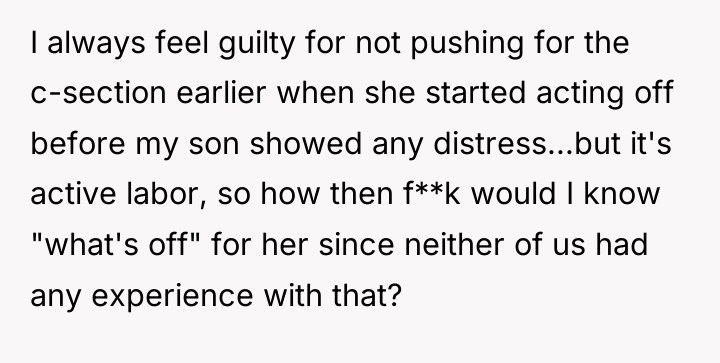
The core issue here is the unsolicited sharing of highly charged, traumatic medical narrative directly to individuals embarking on a significant life event (pregnancy). This behavior bypasses established social boundaries regarding personal medical autonomy. The narrator is projecting their own unresolved guilt—the feeling that they should have pushed for an earlier C-section—onto others. By sharing a story where the outcome was catastrophic (severe autism, immediate emergency), the narrator is effectively injecting fear and imposing their personal risk assessment onto the co-worker’s family planning. This constitutes emotional labor being inappropriately placed upon the recipients, who understandably feel judged or controlled.
The narrator’s actions, while stemming from care, were inappropriate because they imposed a narrative of potential disaster onto a moment of excitement without invitation. A constructive recommendation would be for the narrator to process their lingering guilt regarding their own son’s birth through therapy or personal reflection, rather than attempting to ‘save’ others through fear induction. In the future, if they feel compelled to share, they should wait until directly asked for advice, or keep the information strictly to general, non-specific well-wishes about safe delivery.
AFTER THIS STORY DROPPED, REDDIT WENT INTO MELTDOWN MODE – CHECK OUT WHAT PEOPLE SAID.
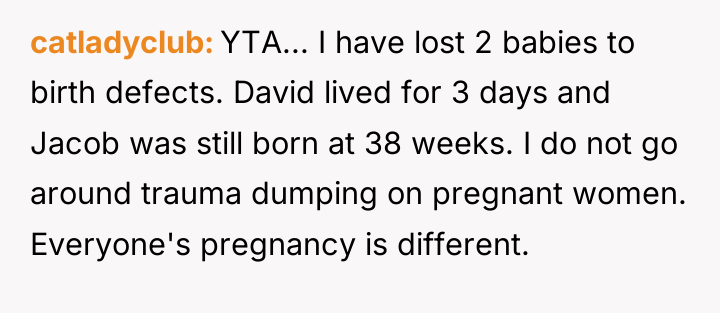
But honestly, no expecting parent wants to have an unsolicited story of a scary birth. This accepted thing needs to stop.
The author is deeply motivated by past trauma and the near-loss of their child, leading them to offer unsolicited, intense birth warnings to expecting parents. This action stems from a desire to prevent others from experiencing similar devastating outcomes, directly conflicting with the expectation from others that personal medical choices should remain private.
Given the author’s clear intent to protect others versus the recipients’ right to autonomy over their birthing plans, the central question becomes: Does the severity of one’s personal trauma justify overriding social norms to deliver unsolicited, fear-inducing cautionary advice regarding major medical decisions?





{kind=link}