
In the quiet shadows of their relationship, a storm of unspoken fears and desires brews. One seeks to embrace their true self, yearning for the transformation that testosterone promises, while the other grapples with the looming changes, afraid of losing the person they thought they knew. Their love stands at a fragile crossroads, caught between acceptance and the daunting unknown.
Beneath the surface lies a profound struggle—not just with hormones and bodies, but with trust and identity. The tension reveals how deeply intertwined love and fear can be, as one battles dysphoria and the need to be seen authentically, and the other wrestles with the intimidating possibility of change, clinging to familiar comforts even as the future demands courage.

AITAH for being upset that my fiancé doesn’t want me taking testosterone

Dr. Ritch C. Savin-Williams, a leading researcher in adolescent development and sexual identity, often emphasizes the critical importance of social support and validation for gender-minority youth navigating identity formation. His work suggests that external pressure or rejection, especially from a primary partner, can significantly increase mental health risks for individuals exploring transition.
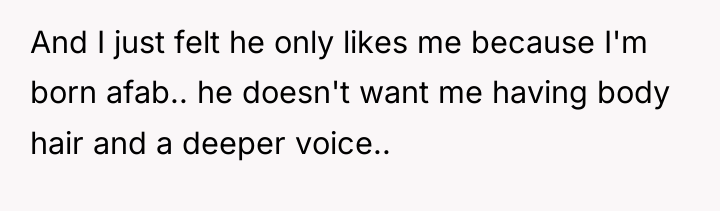
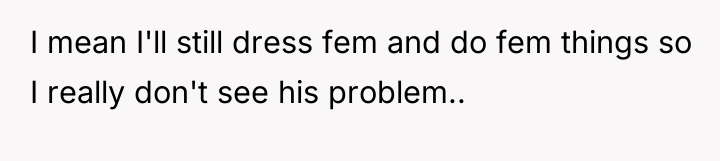
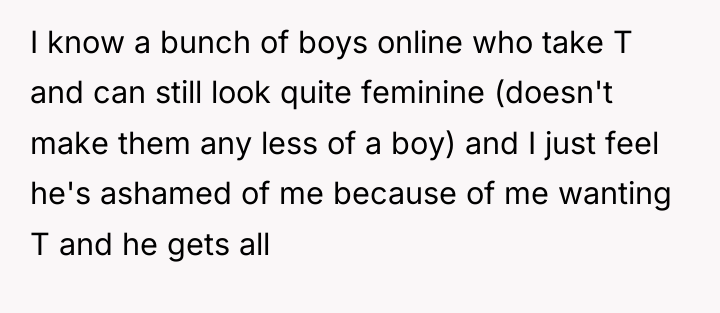
The interaction described reveals a significant misalignment in understanding and priorities. The OP’s motivation for taking Testosterone (T) is rooted in alleviating gender dysphoria and achieving congruence, which is a core psychological need. The partner’s reaction—expressing fear of masculinity, body hair, and voice deepening, and relating these changes to his own fertility concerns (while misrepresenting the risks of estrogen for himself)—suggests that his attraction or commitment might be heavily tied to the OP’s current assigned sex at birth or femininity. This dynamic introduces a power imbalance where the partner’s comfort dictates the acceptable parameters of the OP’s identity exploration.
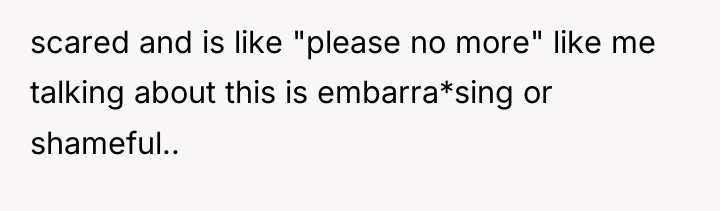
The OP interpreted the partner’s reaction as shame and a feeling that they are only liked for being AFAB. This interpretation is understandable given the partner’s language regarding ‘intimidating’ changes. Constructively, the OP needed a space for open discussion about their dysphoria, not a defensive reaction. For future situations, the OP should prioritize clear, non-apologetic communication about medical decisions as acts of self-care, while firmly setting boundaries against criticism of their identity exploration. If the partner cannot move past aesthetic preferences to support the OP’s fundamental needs, couples counseling focusing on trans-competent communication would be essential.
AFTER THIS STORY DROPPED, REDDIT WENT INTO MELTDOWN MODE – CHECK OUT WHAT PEOPLE SAID.

The original poster (OP) experienced intense emotional distress regarding their gender identity and future medical transition, only to feel invalidated and judged by their partner who expressed fear and disapproval over potential physical changes. This situation highlights a conflict between the OP’s fundamental need for self-affirmation through transition and the partner’s expressed aesthetic and relational expectations.
Is the partner’s concern rooted in genuine care for the OP’s well-being and future, or does it represent an internalized prejudice against masculine traits in a partner, thereby placing the partner’s comfort above the OP’s essential need for bodily autonomy and gender congruence?





{kind=link}